
National Coordinator Explains The ONC “North Star Architecture.” EHRs May Never Be The Same Again.
ONC chief Micky Tripathi spoke at HIMSS22 alongside Dr. Daniel Jernigan, the CDC's deputy director for public health science and surveillance.

ORLANDO, Fla. – During a Tuesday evening Views from the Top session at HIMSS22, National Coordinator for Health IT Micky Tripathi shared the stage with Dr. Daniel Jernigan, Deputy Director For Public Health Science And Surveillance at the Centers for Disease Control and Prevention.
The topic was how the nationwide data exchange system can be shored-up and streamlined to enable more seamless and robust information-sharing with public health agencies – and ease the burden on healthcare providers.
Missing from the presentation, however, was any encouragement that EHRs are on path to function in a manner required to allow the healthtech industry to interoperate between EHRs.
The thrust of the TEFCA improvements described by Tripathi and Jergan centered on improving the public health functionalities of current Electronic Health Record (EHR) systems. To achieve these aims, Tripathi and Jernigan laid out a plan described as the North Star Architecture. We’ve included Tripathi’s graphical representation of the North Star Architecture below.
To explain the North star Architecture one should first understand the Office of the National Coordinator for Health Information Technology (ONC) vision that the US health system will, in its future state, consist of three EHR archetypes: Local State, Tribal, Local, and Territorial (STLT) Hosted, Hybrid and Centrally Hosted EHRs.
Locally Hosted EHRs consist of systems that presently dominate the healthcare information landscape; EHRs like Epic, Cerner and Athena. These are individual EHR instances (typically cloud hosted) that do not take advantage of the proposed ONC Building Blocks. Existing EHRs will, however, be required to share public health aggregated data with the Center for Disease Control and Prevention (CDC) much like a modern EHR / HIE (Health INformation Exchange) framework. The requirement to interoperate with the CDC by pushing USCDI+ (United States Core Data for Interoperability, enhanced consequent to the 21st Century Cures Act) data into the Public Health Aggregated Data repository, looks like back the future. Essentially, the CDC will take on the traditional HIE role and traditional EHRs like Epic and Cerner are required to play along - they must share USCDI+ data with the ONC, and, via the North Star Architecture, every other clinical entity authorized by the patient to access it.
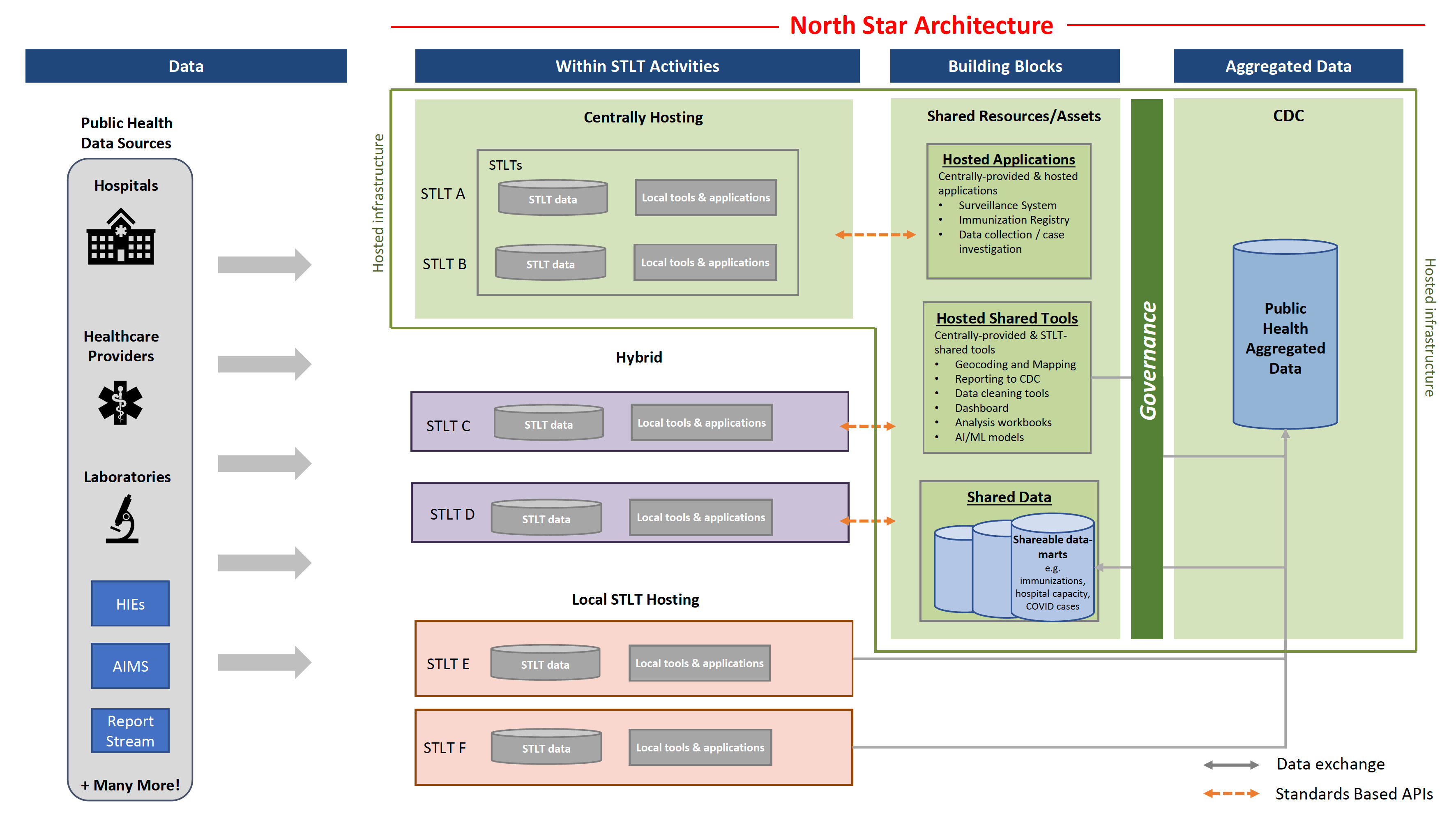
Hybrid EHR systems will look and feel much the same and one can assume they will be derived or evolved from the modern EHR platforms. Hybrid systems, however, will supplementally take advantage of the shared resources and assets the CDC provides: hosted applications, hosted tools and shared data. Like the locally hosted EHRs, they too will be required to push USCDI+ records into the Public Health Aggregated Data repository, but via the North Star Architecture.
Now for the Disruption.
Centrally hosted EHRs will constitute a new EHR archetype entirely. Centrally hosted EHRs will take full advantage of the free ONC North Star Architecture building blocks to the extent that locally hosted EHRs imagined by the ONC will be little more than thin clients built on top of the ONC tool set. Such EHRs don’t exist in the market today but could be disruptive additions to the EHR marketplace.
If “thin client” is not a familiar term for you, a quick primer here. A thin client is a computer or computer application that runs from resources stored on a central server instead of a localized hard drive. Thin clients work by connecting remotely to a server-based computing environment where most applications, sensitive data, and memory, are stored. Thin clients have a number of benefits, including:
Reduced cost
Increased security
More efficient manageability
Scalability
Thin client deployment is more cost effective than deploying regular PCs. Because so much is centralized at the server-side, thin client computing can reduce IT support and licensing costs.
Security can be improved through employing thin clients because the thin client itself is restricted by the server. Thin clients cannot run unauthorized software, and data can’t be copied or saved anywhere except for the server. System monitoring and management is easier based on the centralized server location.
Thin clients can also be simpler to manage, since upgrades, security policies, and more can be managed in the data center instead of on the endpoint machines. This leads to less downtime, increasing productivity among IT staff as well as endpoint machine usersThe ONC NOrth Star Architecture commits the federal government to build, host and maintain the entire “back end” to thin client EHRs of the future - for free. Which then liberates future EHR inventors to, again, focus exclusively on the aspects EHR users actually care about; the User Experience and clinician workflows. This may end up being the most serious threat to the Epic / Cerner duoply in two decades.
Such revolutionary thin client EHRs will be able to compete at far lower cost than the present duopoly of Epic and Cerner due to the fact that ONC will be doing most of the hard work for free. The cost to operate such a thin client EHR would be magnitudes less expensive due to the fact that all data will be written into and drawn out of the free ONC provided data infrastructure. Such EHR products could be created relatively rapidly and cheaply and tap into the unprecedented and free (did I say free?) horsepower of the ONC North Star Architecture Building Blocks.
The ONC does leave one very big missing piece, however, scheduling. Physicians use their EHRs as the source-of-truth for scheduling patient encounters. One of the primary impediments to true EHR interoperability has long been bi-directional schedule integration via FHIR (Fast Healthcare Interoperability Resources) API. Tripathi and ONC have yet to announce any help for future EHR innovators on that critical front.
Despite the lack of vision from ONC and the CDC on scheduling, it will be interesting to see if entrepreneurs and investors jump on this generous offer from the ONC. Could this be 2012 all over again?